Sexually-transmitted infection (STI) - April 12, 2023
The importance of T. vaginalis detection








Trichomonas is underappreciated by healthcare providers and patients alike. Recent advances in diagnostic tests can improve recognition and treatment, leading to better control of this important sexually transmitted disease (STI).
Prevalence of T. vaginalis
A systematic analysis of studies conducted between 2009 and 2016 reports an estimated global prevalence of trichomoniasis of 5.3% in women and 0.6% in men (1.6% and 0.2% in the European region, respectively).1
Clinical presentation
vaginalis is found in the vagina, urethra and paraurethral glands of the female reproductive tract, and in the urethra and sub-preputial sac of the male reproductive tract. Urethral infection by T. vaginalis is present in more than 70% of male partners of females diagnosed with vaginal trichomonas.2
Symptoms of infection with T. vaginalis in women include severe vaginitis (characterised by diffuse malodorous discharge), urethritis (characterised by dysuria) and cervicitis, and, in men, urethritis (characterised by urethral discharge and dysuria).3 A significant number of patients are asymptomatic, with estimates ranging from 25%3 to 50% for women4 and 40–75% of men.3
Trichomoniasis is significantly associated in women with concurrent STIs: 15–28% with chlamydial co-infection and 10% with gonorrhoeal co-infection.5,6
The importance of T. vaginalis detection
Detection and treatment of infected individuals prevents further transmission (via sexual intercourse and vertically from mother to infant at birth). Available effective treatment makes T. vaginalis one of the most curable STIs7 but, left untreated, infection can have long-term health consequences:
Atypical pelvic inflammatory disease (PID)
There is a 4.7-fold increased risk of PID associated with T. vaginalis infections.8 T. vaginalis is also associated with PID in women with a concurrent HIV infection.9
A study of 736 individuals investigating the association between acute and plasma call endometritis, fallopian tube obstruction, herpes simplex virus-2 serology and T. vaginalis infection demonstrated that T. vaginalis infection and HSV-2 serology are associated with PID pathogenesis.10
Infertility
Without detection and treatment, repeated episodes of PID are associated with an increased risk of infertility.11
In men, T. vaginalis causes inflammatory damage or interferes with sperm function and is associated with urethritis, prostatitis, epididymitis and infertility.12
Low birth-weight infants/pre-term births
vaginalis infection is associated with a 1.3-fold increase in the risk of pre-term labour8 and pregnant women infected with T. vaginalis at mid-gestation have been found to be statistically significantly more likely to have a low birth-weight infant or to deliver pre-term.13
Neonatal respiratory infection
There are case study reports that neonates who can acquire T. vaginalis as they pass through the birth canal may develop T. vaginalis-potentiated respiratory disease.14
Risk of HIV sexual transmission and acquisition
The risk of HIV acquisition is increased 2.7-fold when associated with a concurrent T. vaginalis infection.8
Substantial HIV transmission may be attributed to T. vaginalis in African American communities in the US,15 while transmission of HIV may be decreased by reducing T. vaginalis infection.16
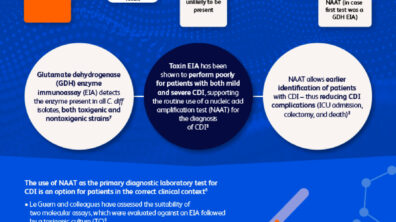
Diagnostic options
Diagnosis and subsequent treatment of trichomonas infections are recommended as infection with T. vaginalis is common and associated with serious potential adverse events.17
The conventional methods for screening are wet mount microscopy and culture techniques. Wet mount microscopy is rapid and inexpensive but is only about 36–75% sensitive compared with culture, which is less again than what can be achieved by nucleic acid amplification tests (NAATs). NAATs can detect a 3–5-fold higher prevalence than wet preparation microscopy. Therefore, NAATs are recommended for T. vaginalis detection in men and women, since they have a higher sensitivity than culture.17
Men with urethritis, or who have a sexual partner with a trichomoniasis infection (due to the high rate of concurrent sexual infection), should be tested.18 T. vaginalis testing likely to increase with the availability of a rapid assays,18 providing epidemiologists with a more accurate picture of trichomoniasis in the community and influencing screening practices for chronic disease prevetion.19
References
- Rowley J, Vander Hoorn S, Korenromp E, Low N, et al. Chlamydia, gonorrhoea, trichomoniasis and syphilis: global prevalence and incidence estimates, 2016. Bull World Health Organ 2019;97:548–62
- Sena AC, Miller WC, Hobbs MM. TV infection in male sexual partners: implication for diagnosis, treatment and prevention. Clin Infect Dis 2007;44:13–22
- Hobbs MM, Sena AC. Modern diagnosis of Trichomonas vaginalis Sex Transm Infect 2013;89:434 – 38
- Allsworth JE, Ratner JA, Peipert JF. 2009. Trichomoniasis and other sexually transmitted infections: results from the 2001-2004 National Health and Nutrition Examination Surveys. Sex Transm Dis 36:738–44.
- Reynolds M, Wilson J. Is Trichomonas vaginalis still a marker for other sexually transmitted infections in women? Int J STD AIDS 1996;7:131–2
- Lo M, Reid M, Brokenshire M. Epidemiological features of women with trichomoniasis in Auckland sexual health clinics: 1998 – 99. NZ Med J 2002;115:U119
- gov. STD Facts – Trichomoniasis. 2021. Available at: https://www.cdc.gov/std/trichomonas/stdfact-trichomoniasis.htm. Accessed August 2021.
- Poole DN, McClelland RS. Global epidemiology of Trichomonas vaginalis. Sex Transm Infect 2013;89:418–22
- Moodley P, Wilkinson D, Conolly C, Moodley J, et al. Trichomonas vaginalisIs Associated with Pelvic Inflammatory Disease in Women Infected with Human Immunodeficiency Virus Clin Infect Dis 2002;34:519–22
- Cherpes TL, et al. 2006. The associations between pelvic inflammatory disease, Trichomonas vaginalis infection, and positive herpes simplex virus type 2 serology. Sex Transm Dis 2006;33:747–52
- nhs.uk/conditions/pelvic-inflammotory-disease-pid/complication
- Fichorova RN. Impact of vaginalis infection on innate immune responses and reproductive outcome. J Reprod Immunol 2009;83:185–9
- Cotch MF, et al. 1997. Trichomonas vaginalis associated with low birth weight and preterm delivery. Sex Transm Dis 1997;24:353–60
- Carter JE, Whithaus KC. Neonatal respiratory tract involvement by Trichomonas vaginalis: a case report and review of the literature. Am J Trop Med Hyg 2008;78:17–9
- Sorvillo F, Smith L, Kerndt P, et al. Trichomonas vaginalis, HIV and African-Americans. Emerg Infect Dis 2001;7:927–32
- Kissinger P, et al. Trichomonas vaginalis treatment reduces vaginal HIV-1 shedding. Sex Transm Dis 2009;36:11–16
- Gaydos CA, Klausner JD, Pant Pai N, Kelly H, et al. Rapid and point-of-care tests for the diagnosis of Trichomonas vaginalis in women and men. Sex Transm Infect 2017;93:S31–S35
- Van Der Pol B. Clinical and Laboratory Testing for Trichomonas vaginalis Infection. Am Soc Microbiol 2016;1:7–12
- Munson KL, Napierala M, Munson E, Schell RF, et al. Screening of Male Patients for Trichomonas vaginalis with Transcription-medicated Amplification in a Community with a High Prevalence of Sexually Transmitted Infection. J Clin Microbiol 2013;51:101–4